– Dr Arun Neopane
Nepal’s health system is often described as underfunded, overstretched and inefficient. These criticisms are familiar, but they do not fully explain why patients remain frustrated, health workers demoralised and governments under pressure despite continued investment. The deeper problem is not only shortage. It is misalignment. 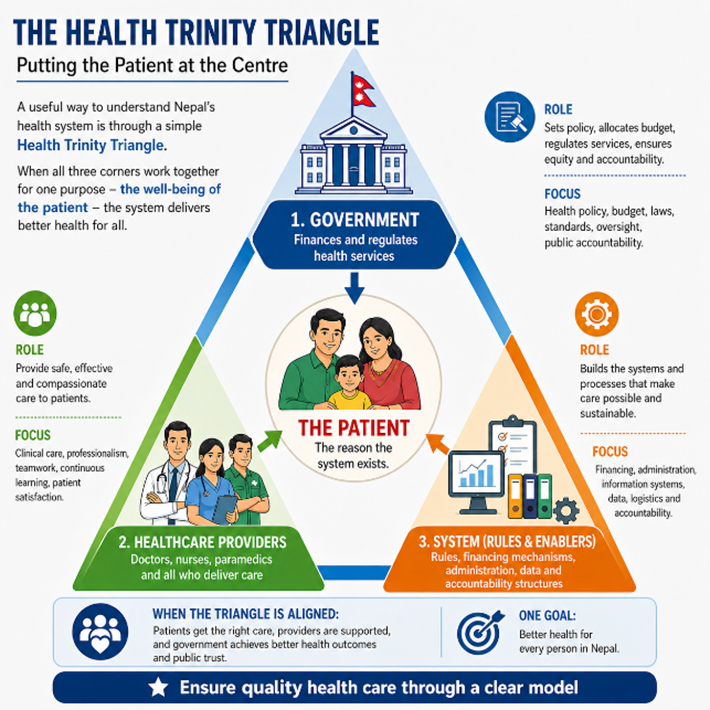 A useful way to understand this is through a simple Health Trinity Triangle. One corner is the government, which finances and regulates services. Another is healthcare providers: doctors, nurses and paramedics who deliver care. The third is the system itself: the rules, financing mechanisms, administration, data and accountability structures that keep services running. At the centre of this triangle should be the patient. That centre is not symbolic. It is the point around which the entire system should function. When the patient remains at the centre, decisions on budgets, staffing, referrals and management naturally move towards better care. When the patient is pushed aside, each corner begins serving its own pressures instead. Governments seek visible outputs such as buildings and equipment. Administrators focus on reports and procedures. Providers struggle under growing workloads. Patients are left navigating delays, rising costs and confusion. When all three corners of the triangle are dissatisfied, the system is no longer holding together. Many Nepalis know this experience well. A patient with fever may move from pharmacy to clinic to hospital before receiving the correct diagnosis. A mother may spend an entire day in a crowded outpatient queue only to be told that a required testing machine is not functioning. Families repeat investigations at multiple centres because records do not follow the patient.
A useful way to understand this is through a simple Health Trinity Triangle. One corner is the government, which finances and regulates services. Another is healthcare providers: doctors, nurses and paramedics who deliver care. The third is the system itself: the rules, financing mechanisms, administration, data and accountability structures that keep services running. At the centre of this triangle should be the patient. That centre is not symbolic. It is the point around which the entire system should function. When the patient remains at the centre, decisions on budgets, staffing, referrals and management naturally move towards better care. When the patient is pushed aside, each corner begins serving its own pressures instead. Governments seek visible outputs such as buildings and equipment. Administrators focus on reports and procedures. Providers struggle under growing workloads. Patients are left navigating delays, rising costs and confusion. When all three corners of the triangle are dissatisfied, the system is no longer holding together. Many Nepalis know this experience well. A patient with fever may move from pharmacy to clinic to hospital before receiving the correct diagnosis. A mother may spend an entire day in a crowded outpatient queue only to be told that a required testing machine is not functioning. Families repeat investigations at multiple centres because records do not follow the patient.
Meanwhile, tertiary hospitals remain crowded with minor illnesses that could have been managed earlier and closer to home. This is why more money alone will not solve the problem. Nepal can build more structures, purchase more equipment and expand budgets, but unless the patient is restored to the centre, outcomes may still disappoint. An unused X-ray machine in a district hospital or a newly painted building without staff does not improve health merely because money was spent. A practical shift is to link payment to results. Instead of funding facilities regardless of performance, payment should follow resolved care whether a safe delivery, treated pneumonia or controlled chronic illness. This shifts the system’s focus from activity to completion of care. It also transforms from equal needs and equal distribution to Targeted Health Equity (THE). In short, if the dislocation of the patient from the centre is the disease, then reorientation is the right treatment.
- Guarantee Timely First Contact: Every citizen whether in the remote districts of Humla or metropolitan Kathmandu should be able to receive qualified initial medical advice within 24 hours through existing health posts, local clinicians and basic telemedicine support. Many illnesses worsen not because treatment is impossible, but because the first step is delayed or unclear. A child with pneumonia in a remote district may arrive critically ill simply because no trained healthcare professional was available to assess the case early enough and treatment was started too late.
- Build Efficient, Interconnected Referral Systems : Referral systems must function as efficient, interconnected nodes. Too many patients bypass lower levels of care, while others are referred upward without coordination. A newborn transferred from a district hospital to Kathmandu without prior confirmation of bed availability may spend hours moving from one hospital to another by ambulance. A bone fracture that could have been treated at a provincial hospital may instead reach an overcrowded central hospital after unnecessary travel and distress. The result is lost time, increased cost and added pressure where it is least needed leaving the patient dissatisfied. A standard referral form, prior confirmation and feedback after transfer would significantly reduce such congestion. These are management fixes, not expensive miracles.
- Use Healthcare Workers Better : The workforce problem is not only one of numerical shortage, but of inefficient utilisation and overload. In many facilities, skilled staff spend excessive time on paperwork, duplicated reporting and non-clinical tasks. Nurses may spend more time completing registers than monitoring patients or providing necessary care. Doctors may lose clinic hours to avoidable administrative work. At the same time, a single doctor or nurse may be responsible for far more patients than is safely manageable. Burnout grows, morale falls and migration becomes more attractive. A system that cannot protect its own workforce cannot sustain itself. Health workers at all levels need fair pay, timely allowances, safe working conditions and recognition for good performance. Rural postings should come with real incentives: housing support, hardship allowances, scholarships, priority for promotion and future training opportunities. Career pathways also matter. Health assistants, nurses, medical officers and specialists should see a clear route for further education and skill development. A nurse in a district hospital should be able to train in emergency or critical care. A medical officer in a rural area should have pathways towards postgraduate specialisation. Paramedics should be able to upgrade their skills in trauma, maternal care or chronic disease management.
- Reward Outcomes, Not Only Activity : Too often, we finance buildings, beds and salaries without asking whether problems were actually solved. Public money should increasingly follow results: safe deliveries, treated pneumonia, completed referrals, controlled chronic illness and reduced waiting times. A municipality that reduces maternal complications or improves immunisation coverage should be recognised more than one that merely inaugurates another structure.
- Ensure Transparency : Every province and municipality should publicly track a few simple indicators: waiting times, medicine stock-outs, referral completion and complaint resolution. What gets measured gets managed. If a district hospital repeatedly runs out of insulin, antibiotics or oxygen, the public should know — and so should those responsible for fixing it.
The encouraging news is that none of this requires a grand constitutional amendment or a massive new budget. Much can be achieved within the current federal framework through discipline, leadership and better use of existing resources. Pilot reforms in one province and one major municipality could demonstrate quick wins within a year. Nepal does not need another fashionable reform slogan. It needs a health system that remembers why it exists. The corners of the triangle should align, and the patient must return to the centre. The simplest test of every decision whether financial, administrative or clinical should be: Did it solve the patient’s problem? If the answer becomes ‘yes’ more often, the system will improve. If not, it may continue to grow in size but not in value.
Dr Arun Kumar Neopane is a senior paediatrician and former Military Health Administrator who retired at the rank of Major General. He is currently President of the Nepal Paediatric Society. Having closely observed Nepal’s health governance system over decades, and having worked in and led major national health emergency responses, he continues to engage actively in national health discourse, particularly in the areas of child health, health system reform, governance and the strategic realignment of healthcare delivery in Nepal.